

作者: Clinical Experts Group, Hamilton Medical
日期: 30.09.2020
Last change: 30.09.2020
(Originally published 02.10.2017) White paper removed from downloads, P/V Tool user guide and quick reference card added. Several methods have been described for performing recruitment maneuvers, with the most commonly used being the sustained inflation method.
Contraindications for RMs are hemodynamic instability, COPD and lung emphysema, bronchopleural fistula, and acute cor pulmonale. Relative contraindications are increased intracranial pressure and pregnancy.
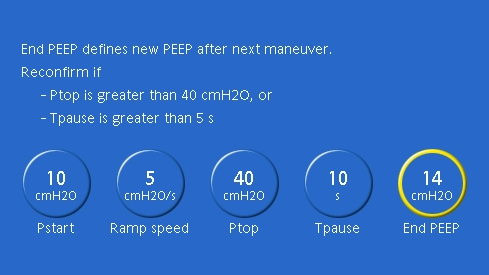
The P/V Tool® Pro on Hamilton Medical ventilators can be used to perform a sustained inflation RM. The clinician needs to set the following (see Figure 1 below):
Note that if esophageal pressure measurement is available, the top pressure can be titrated to target a transpulmonary pressure of 20 cmH2O during the RM (
Before starting the maneuver, the cuff of the endotracheal tube should be overinflated to prevent any air leakage during the maneuver. If using the integrated IntelliCuff pressure controller, this step will be performed automatically.
During the maneuver, the clinician should monitor the mean arterial pressure. A decrease in mean arterial pressure indicates a decrease in cardiac output due to high thoracic pressure. The RM can be stopped at any time in the case of severe hemodynamic compromise.
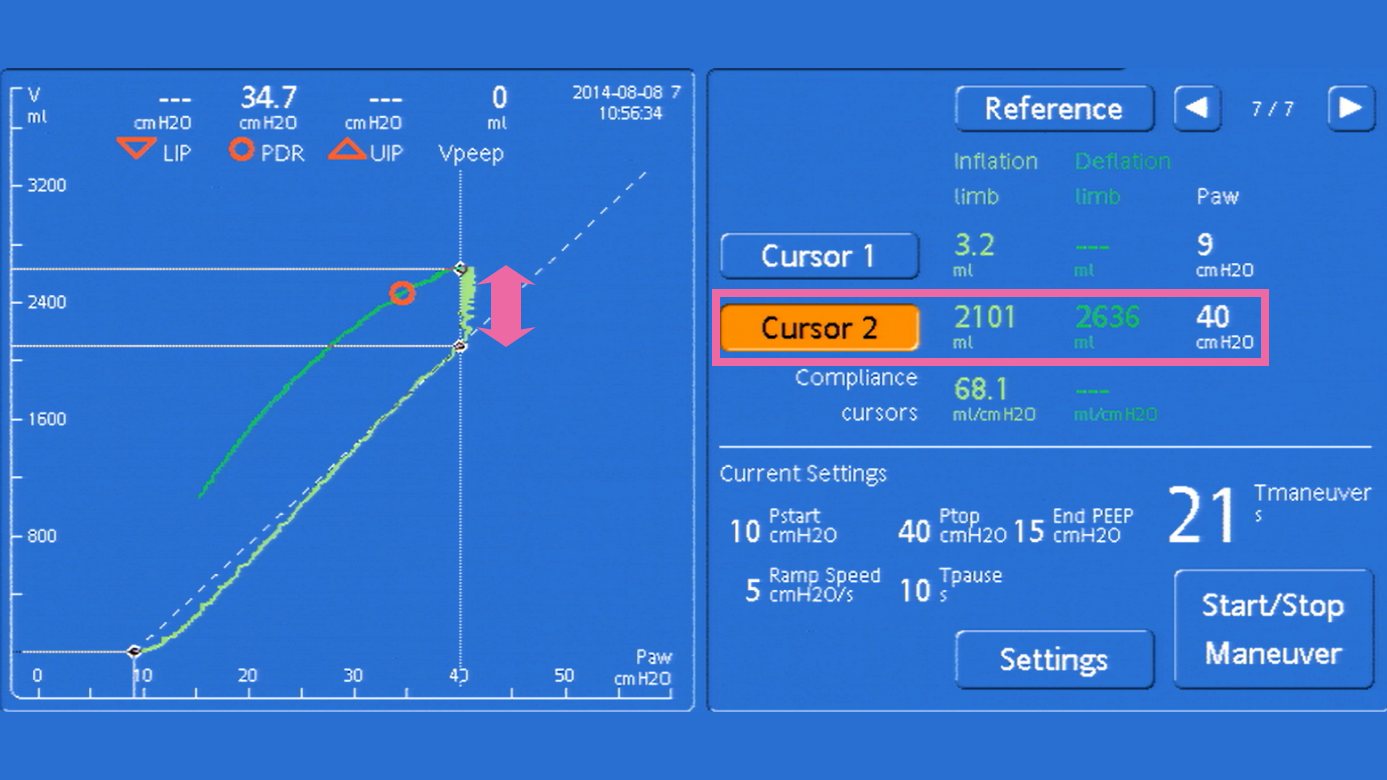
The basis for assessing the efficacy of the RM is the increase in volume during the RM (see Figure 2 below). This volume increase can be measured using the cursor and represents the volume of lung that was reaerated during the RM, assuming there was no air leakage. A volume increase of more than 2 ml/kg predicted body weight (PBW) is considered significant.
A successful RM followed by an appropriate PEEP setting is associated with an increase in static compliance, as well as an improvement in oxygenation and CO2 elimination.
See the documents available for download below. These documents are also available in other languages from our Resource Center.