作者: Clinical Experts Group, Hamilton Medical
日期: 20.04.2020
Hyperoxemia can be defined as an increase in arterial oxygen partial pressure (PaO2) to a level greater than 120 mmHg (16 kPa) (1, 2). It is considered to be moderate for levels ranging between 120 and 200 mmHg, and severe if PaO2 exceeds 200 mmHg (27 kPa) (3). Hyperoxemia is caused by hyperoxia (an increase in oxygen) and occurs in 22% to 50% of mechanically ventilated patients in the ICU (1, 3-6).
Retrospective studies have reported hyperoxemia to be associated with the duration of mechanical ventilation, of the ICU stay and the hospital stay, as well as with ventilator associated pneumonia (
In 2016, results were published from the first large, prospective randomized controlled trial to test whether a conservative protocol for oxygen supplementation to maintain PaO2 within physiological limits could improve outcomes in ICU patients (
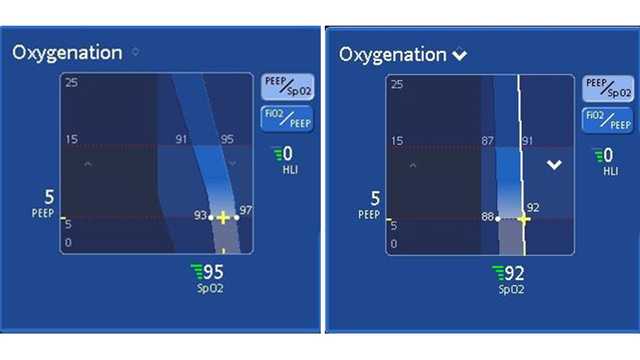
This study shows that avoidance of hyperoxemia is associated with better outcomes, and suggests that clinicians should target physiological ranges of SpO2 and PaO2 in ICU patients. In a pilot, multicenter, randomized controlled trial, a more conservative SpO2 target (88%-92%) was not associated with better outcomes when compared to a normoxia group (
Maintaining SpO2 within target ranges for mechanically ventilated patients requires a number of daily manual adjustments. INTELLiVENT-ASV (
In conclusion, avoiding hyperoxemia and targeting physiological ranges for PaO2 and SpO2 in ICU patients is associated with improved outcomes. A closed loop oxygenation controller may help clinicians to apply this strategy in mechanically ventilated patients, and also reduce the workload for healthcare staff.
Full citations below: (