

作者: Caroline Brown, Branka Cupic
日期: 30.09.2022
在上一期中,我们的床旁建议介绍了使用呼吸机波形识别不同步的起点。
第一步是了解正常的呼吸是什么样的,以及如何识别病人和呼吸机之间的良好同步性。我们介绍了指数递减的概念,以及如何识别吸气努力的开始和良好同步的吸气结束。
下一步是如何识别最常见的较小和较大不同步。
在更仔细地介绍这些之前,我们将回顾构成 Mojoli et al 应用的波形分析系统方法基础的原理。 (
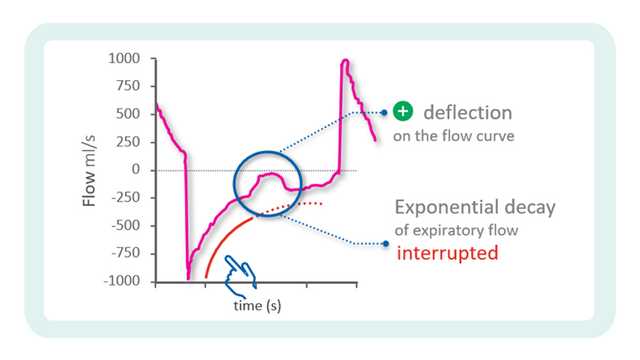
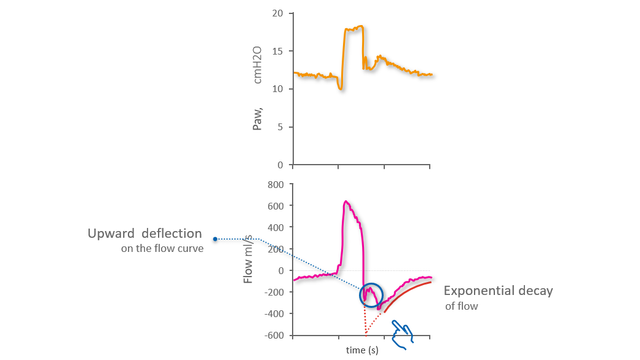
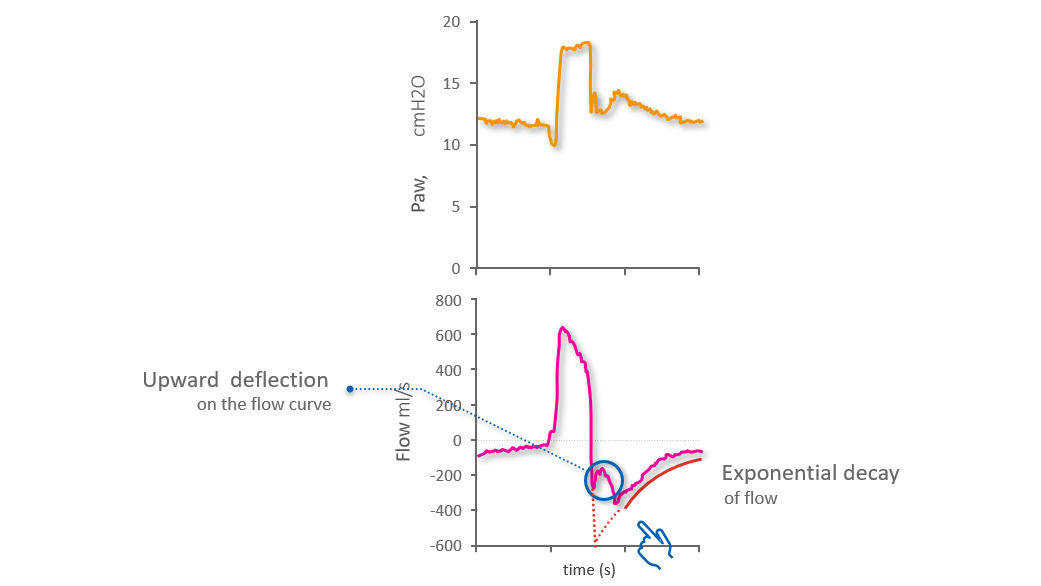
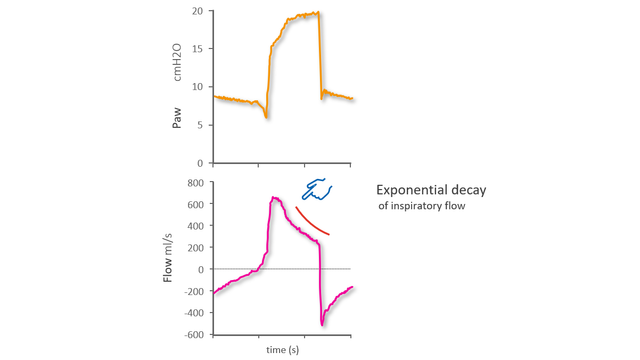
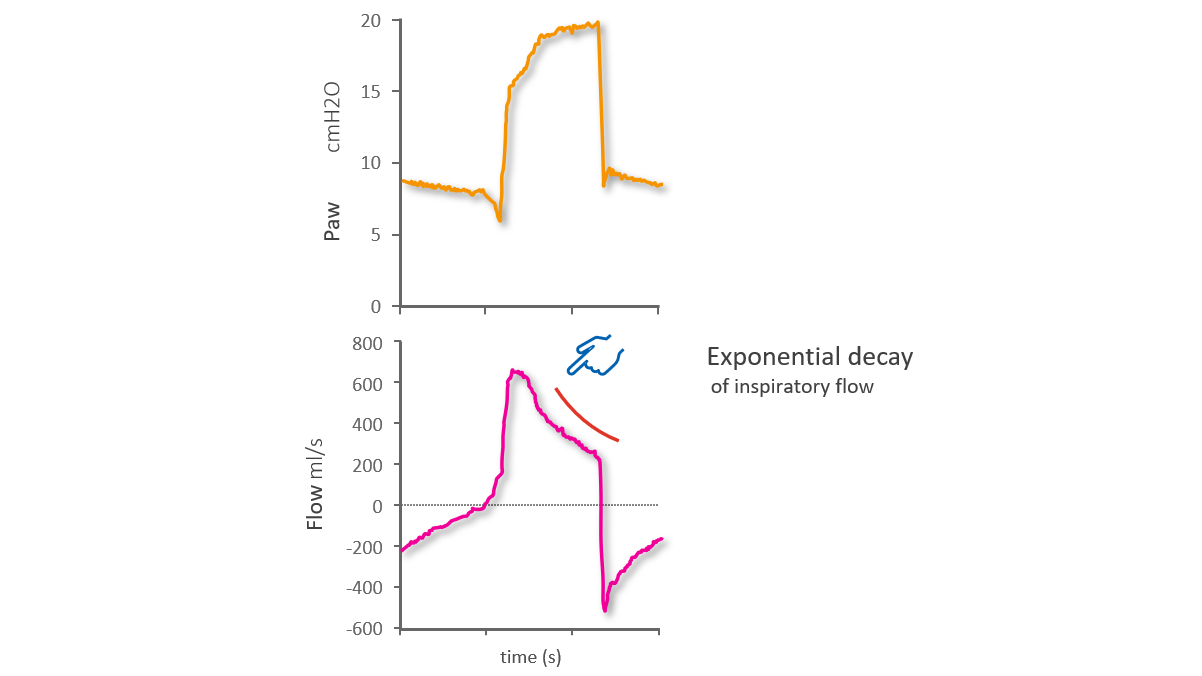
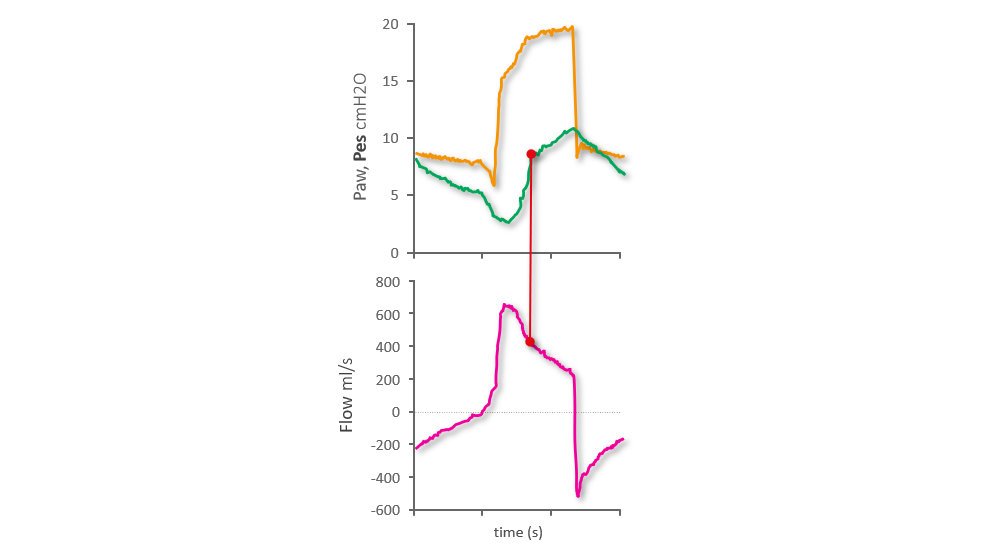
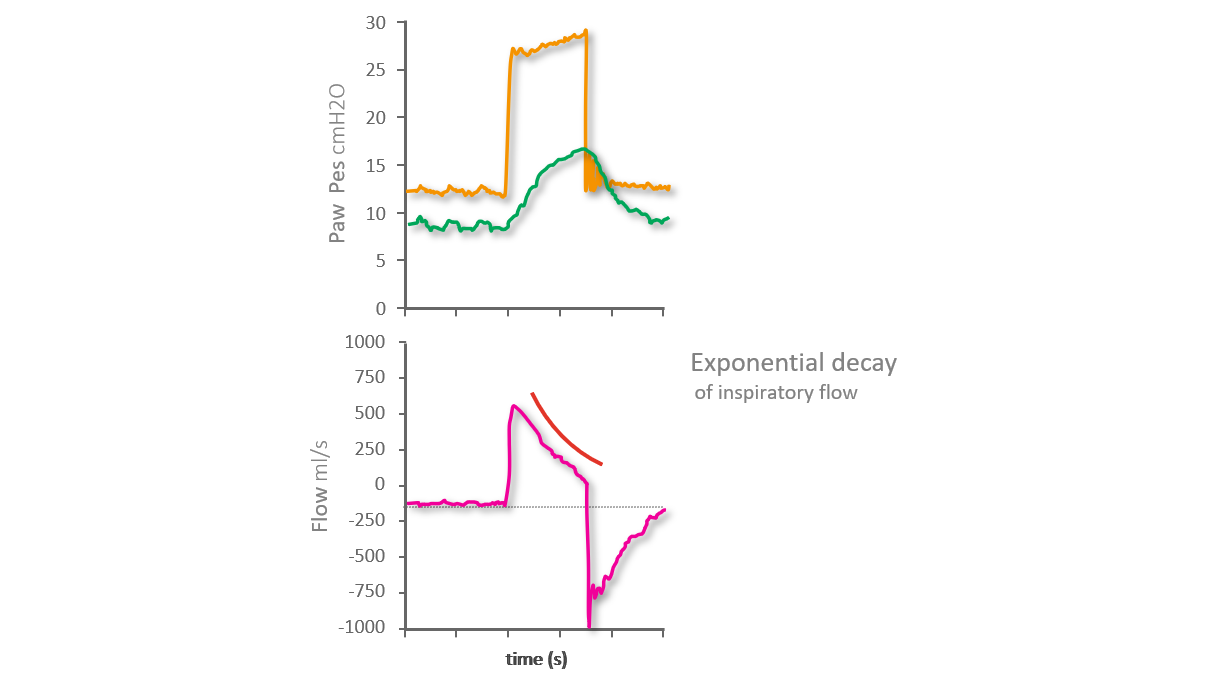
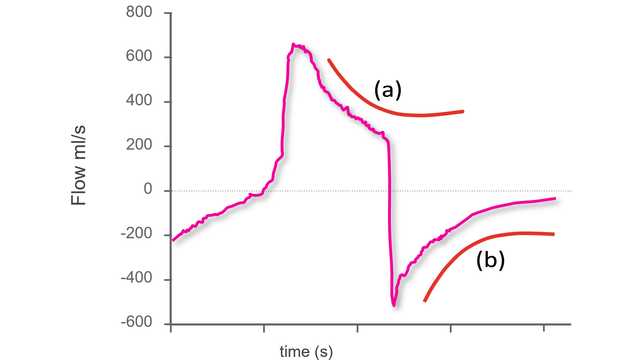
如果病人和呼吸机是同步的,并且切换是最佳的,流量波形将显示呼气开始时的峰值呼气流量,然后是指数递减。提早切换(即呼气在吸气努力结束之前开始),用初始呼气流量的变形来表示:正常的峰值流量被向上偏移所取代,而正常的指数递减开始较晚(见下图 1)。
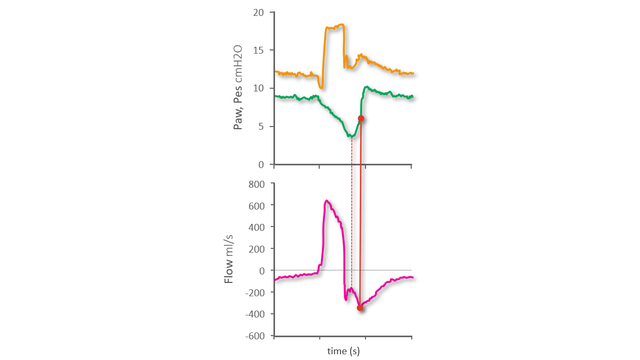
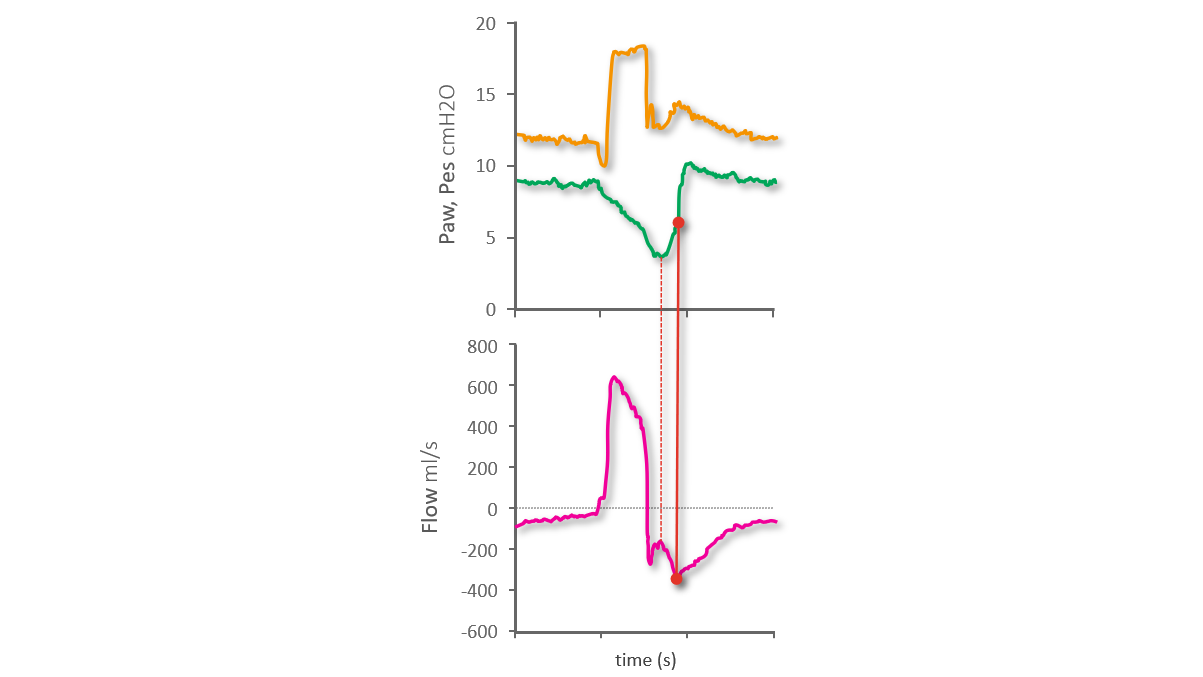
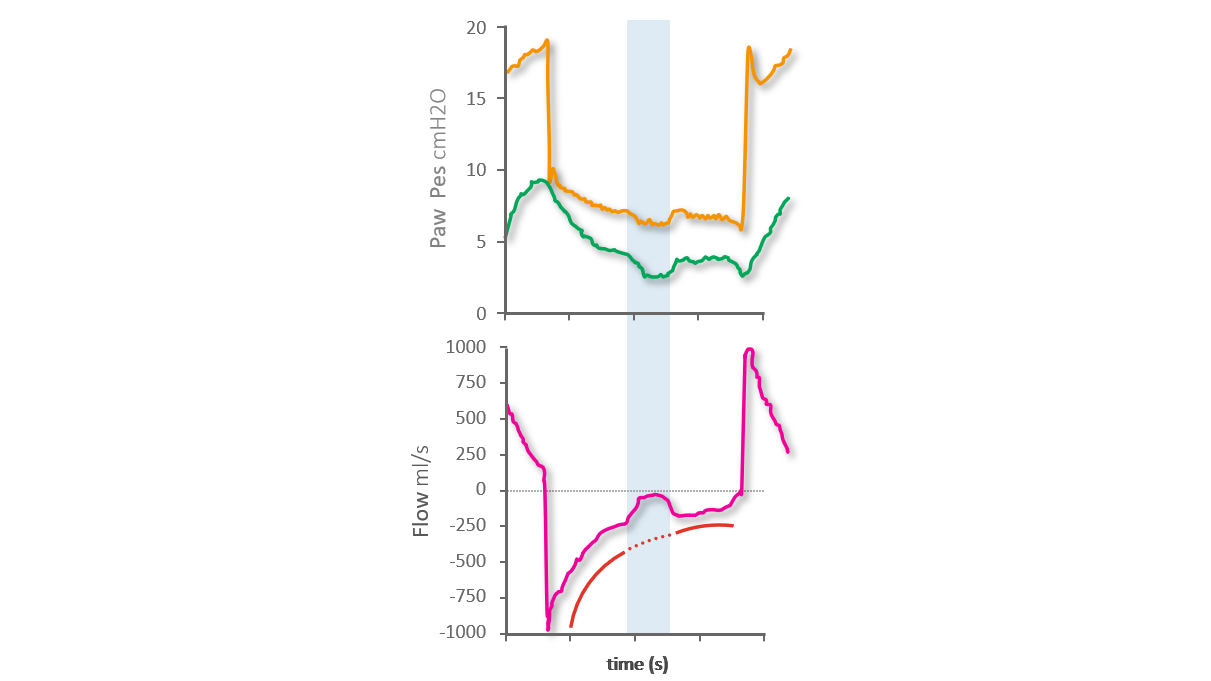
使用食道压 (Pes) 波形作为参考,我们可以看到食道压的最低点(即最大吸气力的点)发生在呼气期间,并与呼气流量的向上偏移相对应。指数流量递减开始较晚,即在吸气努力结束时,如食道压波形上所示(见下图 2)从我们上一个床旁建议中,我们知道食道压在最低点后的快速增加表示吸气肌肉放松,而这个快速增加的中点可以作为吸气结束的参考。
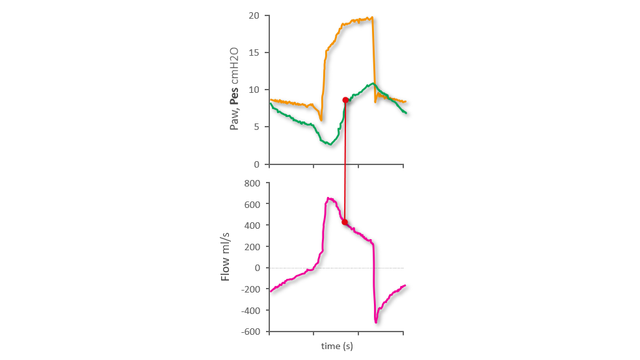
在延迟切换到呼气的情况下,有两个吸气阶段。第一阶段是由吸气肌肉的正常同步拉动和呼吸机的推动引起的,但吸气随后仅由于呼吸机的推动而继续。从而导致被动吸气。您可以从吸气流量在第一阶段后出现的向上凸起的长时间指数递减中在流量波形上识别出这一点(见下图 3)。
在食道压波形上,我们可以看到食道压在最低点后上升的一点,这标志着斜率的明显变化。这一点对应于从同步吸气到随后由延迟切换引起的被动吸气的转变(见下图 4)。
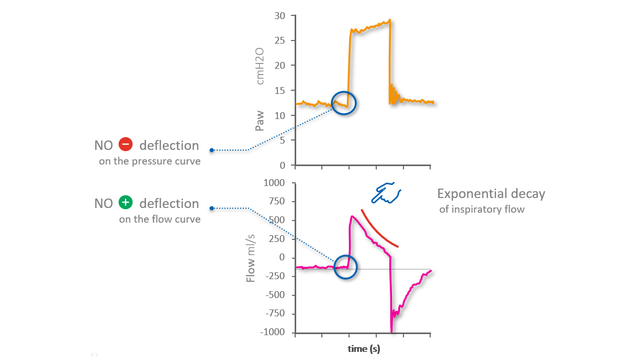
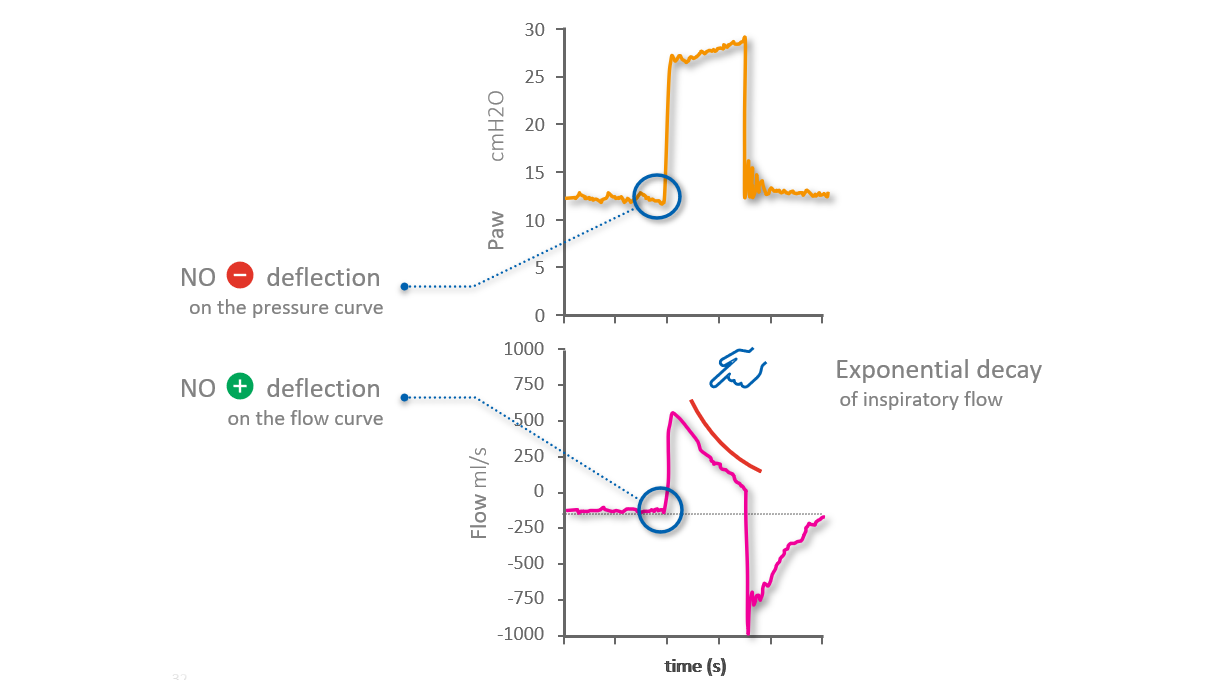
自动触发呼吸是指由呼吸机触发的呼吸,病人无需做出吸气努力。可以通过观察流量和气道压力波形来识别自动触发.没有病人吸气努力的迹象,气道压力没有明显的负偏移,流量也没有明显的正偏移(心脏活动引起的最小振荡除外(见下图 5)。
然而,在吸气流量波形上可以看到自动触发的最强指征,该波形显示一个非常早的峰值,随后是指数递减:整个吸气是由被动吸气导致的。峰值本身的形状也是一个指标:在被动吸气的情况下,峰值是一个尖峰,而在同步吸气时,峰值更弯曲。
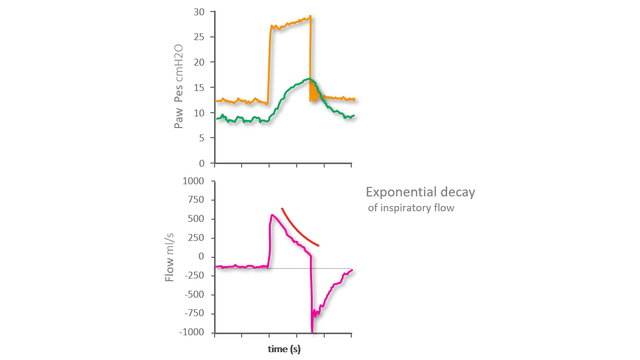
与流量和气道压力波形一样,食道压参考波形上没有可见的负偏移,这通常表示吸气努力的开始(见下图 6)。
无效的吸气努力是指病人在呼吸机呼气阶段做出的吸气努力,但没有被呼吸机识别,因此也没有得到呼吸机的支持。
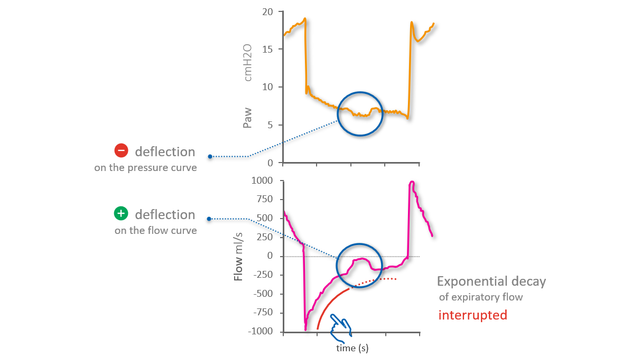
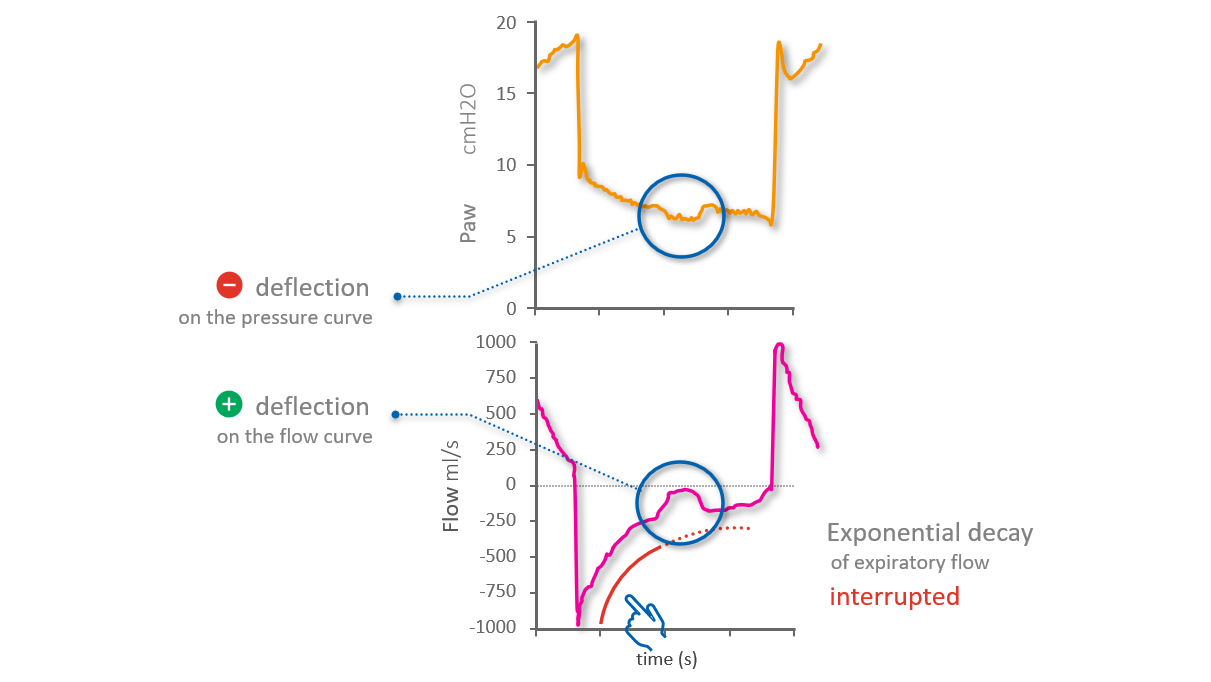
在流量波形上,您可以将无效的努力识别为暂时影响流量正常指数递减的正偏移。在气道压力波形上,同时发生最小负偏移(见下图 7)。
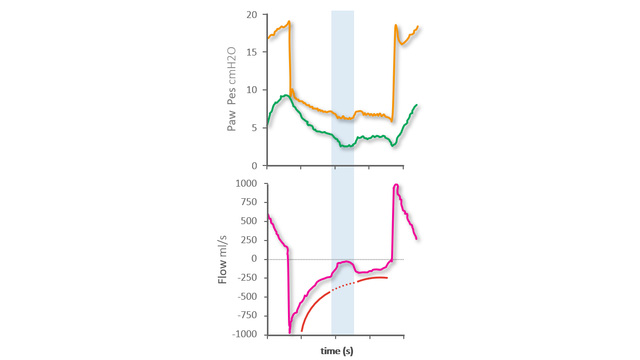
在食道压参考波形上,您可以看到无效吸气努力的开始和结束,显示为食道压的负偏移,影响食道压的正常呼气减少(见下图 8)。

我们的异步参考卡向您概述了最常见的异步性类型、它们的原因以及如何检测它们。
The first step to identifying asynchronies using standard ventilator waveforms is knowing what a synchronous breath looks like during pressure-support ventilation.

Asynchrony between patient and ventilator is a common occurrence in mechanically ventilated patients (1, 2).